Fascia Iliaca or Femoral?
My understanding of this is if we're using a landmark approach, and we use a femoral nerve block the risk of not being in the right soft tissue plane is high. This means that a fascia iliaca block us more likely to be beneficial. The evidence, which I haven't appraised myself, suggests that there's not a significant amount of difference between them all.
Anatomy
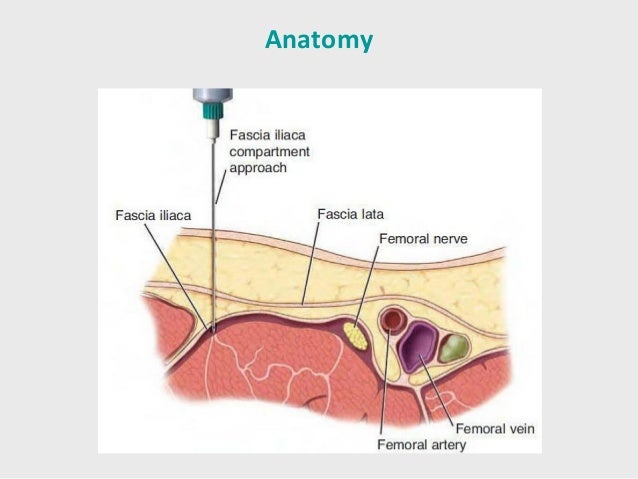
If you look here you can see that the femoral nerve sits, and is enclosed between the fascia lata and the facia iliaca. If you go just lateral to it, you don't know whether you are above or below the fascia iliaca. If you do a fascia iliaca compartment approach, you know you are in the right space.
The podcast from Anatomy for EM is excellent at running through this.
The fascia iliaca compartment contains the three main nerves we are interested in blocking - the femoral nerve, lateral femoral cutaneous and obterator. They provide analgesia for all of the leg except the posterior bit - which the sciatic nerve covers.
Contraindications
· Patient refusal
· Anticoagulation
· Previous femoral bypass surgery
· Inflammation or infection over injection site
· Allergy to local anaesthetics
· Previous femoral bypass surgery
Anaesthetic
We need to use large amounts of local anaesthetic to perform this. 30-40ml should be used for every adult sized patient, and anaesthetic adjusted accordingly.
Our maximum doses are:
Bupivacaine 2mg/kg
Lidocaine 3mg/kg
We normal use 0.25% bupivacaine to provide maximum volume. For a 80kg patient, this would be 160mg which is 60ml of 0.25% bupivacaine. Which is quite a lot. Bupivacaine often works slowly but lasts for a while.
Landmarks
Place one middle finger on the ASIS and the other middle finger on the pubic tubercle.
Draw a line between these two points.
Divide this line into thirds.
Mark the point 1 - 2 cm caudal from the junction of the lateral and middle third.
This is where you are aiming for.
Ultrasound
Ultrasound for blocks isn't yet common practice. I use it to help avoid accidental intravascular injection - put the probe on where I'm going to inject, and double check.
You can see the two fascial layers on ultrasound, and see the local anaesthetic expand. This video demonstrates the use of ultrasound wonderfully.
Complications
Failure
Infection
Accidental intravascular or intraneural injection
Local anaesthetic toxicity
Links and References
http://www.propofology.com/infographs/fascia-iliaca-block
http://learned.rocks/cooked-resourced/2016/8/15/nerve-blocks
http://www.rcemlearning.co.uk/modules/fascia-iliaca-block/
https://songsorstories.com/2016/07/31/pop-pop-phew-sounds-to-go-with-blocks/
http://www.thegasmanhandbook.co.uk/fascia-iliaca-block.html
http://stemlynsblog.org/fib-virgil/
http://bestbets.org/bets/bet.php?id=2673
No comments:
Post a Comment