- Subxiphoid + one other view, normally parasternal long axis
- Identifies pericardial space
- Look at LV RV (?dilated)
- Identifies IVC, looks at diameter and assesses collapsibility
The Probe
If you are using a cardiac probe, the marker (dot) needs to be on the right to give you the views you are used to. This means that mostly, the probe is near the apex of the heart If you are using an abdominal probe (as many of us have to, especially for the subcostal view) the dot will be on the left.
The Anatomy
Remember that the heart doesn't lie exactly vertically. It lies tilted, and slanted. This helps you to think about what you are seeing.
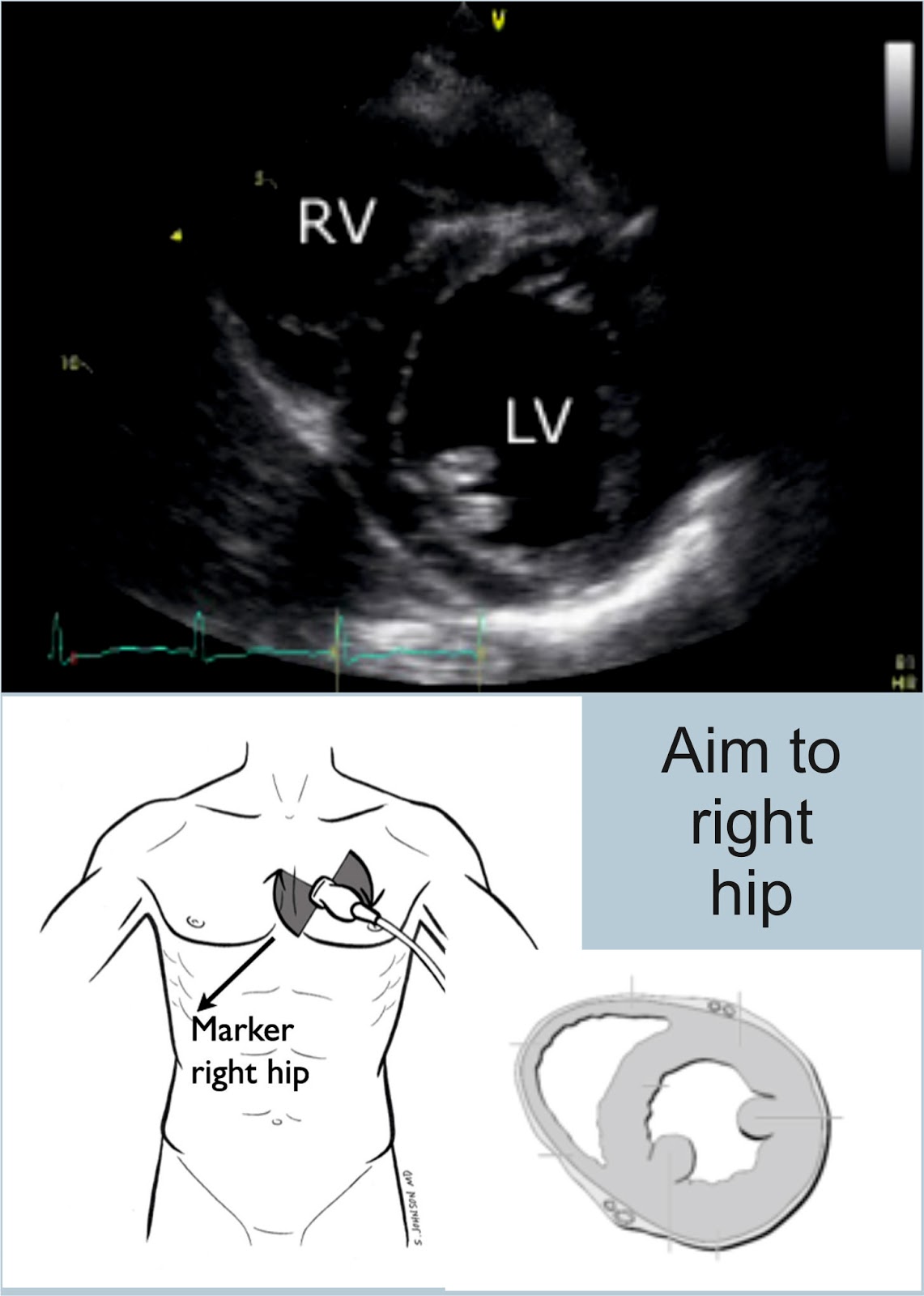
Subxiphoid or Subcostal View
Because the heart is tilted slightly, the probe hits the liver first, then the right hand side of the heart, and then the left hand side - hence the view you get with the right side of the heart at the top, and the left at the bottom.


Fluid normally collects posteriorly. This view is really good for looking at fluid.
Parasternal Long axis
Aim the probe perpendicular to the chest, just to the left of the sternum in the 4-5th IC space (although I was told that the third is better). The marker should be pointing to the top of the patient. Point towards the patient's right shoulder.
This is really good for looking at LV function, and also shows effusions well.


Remember that the right atrium is likely to be hiding behind the aortic outlet.
Parasternal Short Axis
Rotate the probe to look at the patient's left shoulder, keeping the probe marker on the patient's left. This gives you a view at the bottom of the heart - looking at the ventricles.

If you scan at the level of the mitral valve, you get the croissant and doughnut appearance. You also get the fish mouth. This is the view we are aiming to get.
Apical Four and Five Chamber Views
Both of these views have the probe in the same sort of position. To get a five chamber view, you point the probe down a little more to be able to see the aorta. The probe marker is on the patient's left.

IVC
Remember that this will be affected by your probe. Start with a subxiphoid view. Rotate the probe vertically, with the probe marker (using a cardiac probe) at the top. Slide 1-2 cm to the right, and tilt towards the heart. This will give you a view of the liver, with the IVC below it, entering the right atrium.
Measure the heart where the hepatic vein is, or 2-3 cm from the heart edge.
Turn into M mode.
The IVC should collapse on inspiration. If it doesn't, ask the patient to sniff. Measure this as a percentage. If it collapses 25- 50%, they will be fluid tolerant. >50% very likely to be fluid responsive, some say >30%.
I was really struggling to get my head around this anatomy, and one of my collegues drew this brilliant picture for me - and it's mostly clicked. The key I think is thinking about how the heart lies (ie not straight!) and how your probe is looking.



References
http://emergencyultrasound.org.uk/resources/03+Cardiac+views+web.pdf
http://www.rcem.ac.uk/Training-Exams/Training/Ultrasound%20training
http://www.rcem.ac.uk/code/document.asp?ID=5447
https://www.youtube.com/watch?v=oMwgUo6sbyY
https://web.stanford.edu/group/ccm_echocardio/cgi-1bin/mediawiki/index.php/Subcostal_4_chamber_view
http://www.fate-protocol.com/130067GE_Fate_Card.pdf
http://www.smacc.net.au/sonowars-chicago/
http://lifeinthefastlane.com/own-the-echo/


 -
-  -
-